
Humanity’s mental health crisis is not an abstraction. It is visible in the student who cannot sleep before an examination, the caregiver whose exhaustion has become chronic, the employee who appears productive while privately struggling with panic, and the older adult whose grief has narrowed life into isolation. These experiences differ in cause and severity, but they share a painful feature: distress can become so closely fused with identity that a passing mental state begins to feel like the whole person.
The epidemiological scale is formidable. The 2023 Global Burden of Disease analysis estimated that 1.17 billion people were living with one of 12 assessed mental disorders. That represented a 95.5% increase in the number of prevalent cases since 1990. More importantly, after adjusting for population growth and changing age structure, the prevalence rate still rose by an estimated 24.2%. Mental disorders accounted for approximately 171 million disability-adjusted life-years and were the world’s leading cause of years lived with disability. Anxiety disorders and major depressive disorder were among the largest contributors to this burden, according to the 2026 GBD analysis published in The Lancet.
The distinction between case counts and age-standardised rates matters. A near doubling of cases does not mean that every individual’s probability of illness has doubled. Population growth, ageing, improved detection, diagnostic practices, conflict, poverty, social disruption, the COVID-19 pandemic and genuine changes in prevalence all influence the total. Responsible interpretation therefore requires both urgency and statistical restraint.
India carries a substantial share of this burden. A state-level analysis in The Lancet Psychiatry estimated that 197.3 million people in India experienced mental disorders in 2017, including approximately 45.7 million with depressive disorders and 44.9 million with anxiety disorders. In practical terms, about one in seven Indians was affected by a mental disorder of varying severity. The proportion of India’s total disease burden attributable to mental disorders rose from 2.5% in 1990 to 4.7% in 2017, although prevalence and access to care varied markedly between states. These estimates are detailed in the India State-Level Disease Burden Initiative.
Self-reported well-being surveys reveal a related, though methodologically different, picture. The India Health Quotient 2026 survey, conducted among 2,600 urban respondents in 16 cities, reported that 82% experienced stress and 14% regarded it as unmanageable. Such a commissioned urban survey cannot establish national psychiatric prevalence, and stress is not synonymous with a diagnosable disorder. It nevertheless captures an important lived reality: many people remain outwardly functional while sleep, attention, relationships, physical health and hope are quietly deteriorating.
The Question Beneath the Symptoms
Modern psychiatry and psychology have developed sophisticated accounts of mental suffering. Contemporary care is not limited to suppressing symptoms; it may address trauma, attachment, cognition, behaviour, neurobiology, family systems, occupational stress, poverty, discrimination, sleep, substance use and physical illness. Psychotherapy, medication, social support, rehabilitation and preventive interventions can all be essential. Any credible engagement with ancient wisdom must begin by recognising these achievements rather than setting tradition and science against one another.
A further question nevertheless remains relevant: what happens when a thought, emotion or bodily sensation is treated not merely as an experience, but as an exhaustive statement of identity? A thought such as “I am a failure” may initially be a brief mental event. Repetition, emotional arousal and selective attention can gradually turn it into a seemingly unquestionable description of the person. Anxiety may shift from “anxiety is present” to “I am anxious”; grief may become “I am broken”; anger may become “I am an angry person.” Grammar then reveals a psychological fusion: a changing state has been converted into a fixed self.
Ancient Indian contemplative traditions examined this fusion through concepts such as Avidyā, asmitā, attachment, aversion, discernment, equanimity and witnessing awareness. These concepts are philosophical and soteriological; they are not substitutes for psychiatric diagnoses. Avidyā should not be presented as the sole medical cause of depression, schizophrenia, bipolar disorder, post-traumatic stress or any other condition. Rather, it offers a phenomenological account of how suffering may be intensified when awareness becomes entangled with mental content.
This distinction prevents two errors. The first is reductionism: treating every form of suffering as a chemical imbalance or cognitive defect while ignoring meaning and identity. The second is spiritual bypassing: treating poverty, violence, illness, bereavement or psychiatric symptoms as mere failures of awareness. Mental suffering can have biological, interpersonal, structural and contemplative dimensions at the same time. Explanations at one level do not cancel explanations at another.
The Ancient Diagnosis: Avidyā and Misidentification
In classical Yoga, Avidyā is not simply a lack of information. It refers to a fundamental error in seeing: the unstable is treated as stable, the conditioned as absolute and the contents of awareness as the entirety of the Self. This account does not claim that thoughts and emotions should disappear. It asks whether they are being perceived accurately—as changing events—or being mistaken for an unchanging identity.
Patañjali’s opening account of Yoga places this relationship between awareness and mental fluctuation at the centre of practice:
योगश्चित्तवृत्तिनिरोधः । तदा द्रष्टुः स्वरूपेऽवस्थानम् । वृत्तिसारूप्यमितरत्र ॥
(Yoga is the stilling of the fluctuations of the mind. Then the Seer abides in its own nature. At other times, it becomes identified with those fluctuations. (Yoga Sūtras of Patañjali 1.2–1.4))
The passage is sometimes misunderstood as a demand to eliminate thought. Yet nirodha is better approached as disciplined regulation, settling or mastery of mental activity, not neurological blankness. A healthy mind must remember, plan, imagine, discriminate and respond. The problem is not that a thought appears; the problem arises when awareness loses all perspective on the thought and reacts as though its content were complete, permanent and unquestionably true.
A familiar episode illustrates the mechanism. An employee receives a terse message requesting an urgent meeting. Before any facts are known, the body tightens, the mind predicts dismissal, and memories of earlier criticism become newly vivid. Within seconds, a short message has generated a story about competence, security and worth. Witnessing awareness does not deny the meeting or force the fear away. It recognises the sequence: a message was received; threat predictions arose; the chest tightened; an old narrative became active; further information is still required. That small recovery of sequence can restore choice.
The Yoga Sūtras: From Kleśa to Clarity
The Yoga Sūtras describe five kleśas, or afflictive processes: Avidyā, asmitā, rāga, dveṣa and abhiniveśa. These are commonly rendered as misapprehension, egoic identification, attachment, aversion and clinging to continuity or life. They form a dynamic system. Misapprehension supports a rigid sense of “I”; that identity pursues experiences believed to secure it, rejects experiences perceived to threaten it and fears its own disruption.
अिवद्याक्षेत्रमुत्तरेषां प्रसुप्ततनुिविच्छन्नोदाराणाम्
(Avidyā (ignorance) is the source field for the remaining four kleśas- asmitā (egoism), rāga (attachment), dveṣa (aversion), and abhiniveśa (clinging to life). (Yoga Sūtras of Patañjali 2.3-2.5))
The cited line is conventionally associated with Yoga Sūtra 2.4 and belongs to the sequence developed in 2.3–2.5. Its agricultural metaphor is useful: Avidyā is a field in which other afflictions may remain dormant, weakened, interrupted or fully active. This is not a binary model in which a person is either enlightened or ignorant. It describes fluctuating tendencies whose intensity changes with context, habit and practice.
Yoga therefore offers more than introspective observation. Its classical discipline includes ethical restraints, constructive observances, embodied posture, regulation of breath, management of sensory attention, concentration, meditation and contemplative absorption. This broader architecture matters clinically. Witnessing divorced from ethics, sleep, bodily regulation and conduct can become an abstract exercise. In the classical model, clarity is stabilised through an integrated way of living.
The Bhagavad Gītā: Kṣetra, Kṣetrajña and Action
The Bhagavad Gītā distinguishes the Kṣetra, or Field, from the Kṣetrajña, the Knower of the Field. The Field includes embodiment and the changing domain of experience. Thoughts, emotions, memories, social roles and bodily states can all be understood as occurring within this knowable field. The distinction does not demean the body; it prevents the known from being confused with the capacity by which it is known.
इदं शरीरं कौन्तेय क्षेत्रमित्यभिधीयते । एतद्यो वेत्ति तं प्राहुः क्षेत्रज्ञ इति तद्विदः ॥
(This body, O Arjuna, is called the Field. One who knows this field is called the Knower of the Field. (Bhagavad Gītā 13.2))
Crucially, the Gītā situates insight within action. Arjuna is not advised to escape responsibility by declaring the world unreal. He is taught to act with discernment while loosening the compulsive dependence of identity on success, failure, praise and blame. This is expressed through Samatva, a cultivated steadiness that permits engagement without psychological captivity.
योगस्थः कुरु कर्माणि सङ्गं त्यक्त्वा धनञ्जय । सिद्ध्यसिद्ध्योः समो भूत्वा समत्वं योग उच्यते ॥
(Established in Yoga, act. Remaining equal in success and failure – this equanimity is called Yoga. (Bhagavad Gītā 2.48))
Samatva is not emotional flatness. A person may feel grief, delight, fear or disappointment while retaining the ability to choose a proportionate response. In modern psychological vocabulary, aspects of this capacity resemble emotional regulation, distress tolerance and cognitive flexibility. The resemblance is illuminating, but it does not make the concepts identical: the Gītā places equanimity within a larger account of Yoga, duty, knowledge and liberation.
Ayurveda: Prajñāparādha Without Blame
Ayurveda contributes another lens through Prajñāparādha, often translated as an error or transgression of discernment. Classical discussions connect it with disturbances of dhī, dhṛti and smṛti—understanding, restraint and memory. A person may know that a pattern is harmful yet repeatedly enact it because immediate impulse eclipses remembered knowledge. Chronic overwork, compulsive consumption, destructive conflict and persistent disregard of bodily limits can all illustrate this gap between knowing and living.
It would be inaccurate to reduce the Ayurvedic account of illness to Prajñāparādha alone. Classical Ayurveda also considers constitution, diet, behaviour, environment, time, sensory contact and other causal conditions. Its value here lies in emphasising that health depends partly on discernment embodied in daily choices, not merely on abstract information.
आत्मानमेव मन्येत कर्तारं सुखदुःखयोः| तस्माच्छ्रेयस्करं मार्गं प्रतिपद्येत नो त्रसेत्||
(One should hold oneself responsible for one’s happiness and misery. Therefore, one should walk the path of well-being without fear. (Caraka Saṃhitā, Nidāna Sthāna 7.22))
In a mental health context, “responsible” must mean capable of meaningful agency, not morally culpable for illness. A traumatised person did not choose the traumatic event. A person with bipolar disorder did not create the condition through insufficient discipline. Someone living under violence or deprivation cannot meditate away an unsafe environment. Discernment becomes therapeutic only when it is joined with compassion, appropriate treatment and recognition of circumstances.
The Tamil Siddha Tradition: The Body as Temple
The Tamil Siddha tradition supplies an essential corrective to interpretations that turn witnessing into rejection of the body. Thirumūlar describes a movement from disdain for embodiment to reverence after discovering sacred reality within it. Awareness and embodiment are not presented as enemies; the body becomes a locus of care and realisation.
உடம்பினை முன்னம் இழுக்கென் றிருந்தேன்
உடம்பினுக் குள்ளே யுறுபொருள் கண்டேன்
உடம்புளே உத்தமன் கோயில்கொண் டான் என்று
உடம்பினை யானிருந் தோம்புகின் றேனே
(Once I regarded the body as impure. Then I discovered the Supreme Reality within it. Realizing that the Divine had made this body Its temple, I began to care for it with reverence. (Thirumantiram 725))
This embodied emphasis has direct relevance to mental health. Adequate sleep, nutrition, movement, medical evaluation, safe relationships and regulation of the nervous system are not inferior preliminaries to “higher” awareness. They are conditions that often make sustained attention possible. A practice that encourages contempt for pain, hunger, medication or physical limitation has departed from the reverence articulated in this verse.
A Dharmic Conversation Without Erasing Difference
The wider family of Hindu, Buddhist, Jain and Sikh traditions contains multiple disciplines of attention, ethical restraint, non-attachment, compassion and remembrance. These traditions can enrich one another without being collapsed into a single doctrine. Intellectual unity is strongest when genuine differences are acknowledged rather than concealed.
Many Buddhist traditions cultivate mindful observation of sensations, feelings and mental states while emphasising impermanence and non-self. That framework should not be casually equated with a Vedāntic witnessing Self; the metaphysical claims differ. The practical recognition that thoughts can be observed without possession, however, provides a meaningful point of dialogue.
Jain disciplines such as sāmāyika cultivate equanimity, careful awareness and temporary withdrawal from harmful reactivity. Jain accounts of the soul, karma and liberation remain philosophically distinctive, yet their emphasis on nonviolence extends psychological observation into speech, conduct and responsibility toward other beings.
Sikh traditions centre remembrance of the Divine, ethical labour, service, humility and alignment with hukam. Their approach resists a purely private spirituality: inner steadiness is expressed through truthful action and seva. This offers an important reminder that mental well-being is relational and communal, not merely an individual achievement.
Across these traditions, a shared practical principle can be stated cautiously: attention need not be enslaved by every passing mental event, and freedom should deepen compassion rather than withdrawal. The traditions disagree about the ultimate nature of self and reality, but they can still participate in a respectful civilisational conversation about suffering, conduct and liberation.
The Witness Within: What Sākṣī Bhāva Means
Sākṣī Bhāva is commonly rendered as the disposition or stance of the witness. It refers to awareness of experience without total identification with what is being experienced. The witness remains present to thought, emotion and sensation while recognising their changing character. This is participation with perspective, not retreat from life.
The analogy of a film clarifies the shift. A viewer may laugh, cry and tense with fear while absorbed in a story. The experience is real, but the viewer is not literally the character on the screen. Remembering this fact does not end the film or abolish emotion. It creates a small interval between the story and the one who is aware of it.
Mental life often operates in a similar way. Images, predictions and memories appear on an inner screen. When a frightening thought is believed without perspective, the nervous system may respond as though the predicted catastrophe were already occurring. Witnessing introduces a crucial distinction: the thought is real as a mental event, but its proposition may still be incomplete, exaggerated or false.
The shift can be heard in language. “I am worthless” becomes “a thought of worthlessness is present.” “I cannot survive this feeling” becomes “the mind is predicting that this feeling will be intolerable.” “I am anger” becomes “anger is moving through the body and preparing it for action.” These formulations do not invalidate distress. They convert an identity claim into an observable process.
That conversion can create room for inquiry. What triggered the state? Which bodily signals accompany it? What evidence supports the thought? Which earlier experience is being reactivated? What action accords with present values rather than immediate impulse? The witness is clinically useful when it leads to more accurate contact with reality and more skilful action.
Witnessing Is Not Suppression, Avoidance or Dissociation
Several superficially similar processes must be distinguished. Suppression attempts to force an experience out of awareness. Experiential avoidance organises behaviour around escaping unwanted internal states. Intellectualisation analyses an emotion while avoiding direct contact with it. Witnessing, by contrast, permits the experience to be known while reducing automatic obedience to it.
Dissociation may involve numbness, unreality, detachment from the body, discontinuities in memory or a disturbing sense of observing oneself from outside. Witnessing should increase grounded presence, sensory clarity and voluntary choice. If a practice produces escalating unreality, panic, memory gaps or loss of functioning, that response should not be romanticised as spiritual attainment. It may require modification of the practice and assessment by a qualified mental health professional.
Three practical tests help preserve the distinction. First, healthy witnessing generally increases contact with present sensory information rather than making the world feel unreal. Second, it broadens behavioural choice rather than producing paralysis. Third, it supports care for the body and relationships rather than indifference to them. A contemplative stance that fails these tests may be avoidance wearing spiritual language.
Where Ancient Insight Meets Modern Psychology
Contemporary psychology describes related capacities through terms such as decentering, meta-awareness, cognitive distancing, cognitive defusion, psychological flexibility and self-as-context. A critical review of decentering research identified three recurring processes: awareness of mental activity, reduced identification with internal experience and diminished automatic reactivity to thought content. This model closely resembles important functional aspects of witnessing, although it makes no necessary metaphysical claim about consciousness.
Cognitive therapy helps a person examine the evidence, assumptions and behavioural consequences associated with a thought. Acceptance and Commitment Therapy often uses cognitive defusion to alter the thought’s functional grip rather than debating every proposition. Mindfulness-Based Cognitive Therapy trains recognition of depressive thinking as a recurring mental pattern, especially in people vulnerable to relapse. Metacognitive approaches focus on beliefs about thinking itself, including the conviction that worry is uncontrollable or necessary.
These therapies do not simply repeat ancient teachings under new names. They use operational definitions, structured protocols, clinical assessment and measurable outcomes. Evidence also varies by population, intervention and comparator. A 2024 meta-analysis of 21 randomised trials found that Mindfulness-Based Cognitive Therapy produced moderate reductions in anxiety and depressive symptoms, with gains generally maintained at follow-up. Such findings support clinical usefulness; they do not establish meditation as universally effective or superior to all other treatments.
The philosophical difference remains important. Most psychological models treat observing as a trainable metacognitive capacity or functional perspective. Many Indian traditions regard witnessing as more fundamental—as an aspect, expression or nature of consciousness itself. Science can investigate reports, behaviour, physiology and neural correlates, but it cannot settle that ontological question merely by showing a change in a brain scan.
The strongest bridge therefore rests on functional convergence rather than forced equivalence. Both domains can examine whether reduced fusion with thought improves emotional regulation, behavioural flexibility and well-being. They need not pretend that Sākṣī Bhāva, decentering and self-as-context are interchangeable in history, purpose or metaphysics.
From Philosophy to a Grounded Practice
A safe introductory practice can cultivate perspective without denying embodiment. It should be brief, voluntary and adapted to the individual. The objective is not to achieve a special state, eliminate thought or prove a doctrine. It is to notice experience accurately and recover a degree of freedom in responding.
1. Orient to the present. The practitioner may begin with open eyes and identify several neutral features of the environment: colours, sounds, contact with the floor and the location of exits. This signals that contemplative attention is occurring in a specific, safe-enough setting rather than in an abstract mental space.
2. Establish an embodied base. Attention can rest on the feet, hands, sitting bones or natural movement of breathing. Breath should not be forced. For people whose breath is associated with panic or trauma, external sound or contact with the ground may be a better anchor.
3. Recognise events by category. When experience arises, it can be labelled gently: thinking, remembering, planning, fear, tightness, sadness or urge. A label should be light enough to aid recognition without turning the session into constant commentary.
4. Change the relationship expressed in language. Instead of repeating “I will fail,” the practitioner may note, “the mind is producing a prediction of failure.” Instead of “this anxiety must stop,” the observation becomes, “anxiety is present, and its intensity can be tracked.” This is not positive thinking; it is grammatical accuracy about the difference between a person and a mental event.
5. Include the body. The location, movement, temperature and intensity of sensation can be observed without assuming that every sensation is dangerous. If distress becomes overwhelming, attention should return to external orientation, movement or supportive contact. The practice is not a test of endurance.
6. Introduce inquiry carefully. The Upaniṣadic formula neti neti (नेति नेति)—“not this, not this”—invites discernment about what the Self is not. In a psychologically grounded adaptation, a thought can be recognised as something known rather than the totality of the knower. The body can be recognised as experienced without being neglected or despised. The inquiry should deepen care and clarity, not generate alienation.
Statements such as “I am not the body” and “I am not even the mind” are therefore best approached as contemplative prompts within their philosophical context, not literal instructions to disown embodiment or cognition. For a person vulnerable to depersonalisation, psychosis or severe dissociation, these formulations may be destabilising. A safer inquiry may be: “Is this thought the whole of the person, or is it one event being experienced now?”
7. Widen awareness. After observing one dominant event, attention can expand to include sounds, posture, breath, emotion and space together. This reduces tunnel vision and demonstrates that even intense distress is usually one component of a larger field of experience.
8. Re-enter purposeful action. The session should end with a concrete next step: drinking water, making a clinical appointment, returning a message, resting, apologising, setting a boundary or completing one manageable task. Witnessing becomes psychologically meaningful when it improves engagement with life.
A brief record can strengthen learning. The practitioner may note the trigger, dominant thought, bodily response, action urge, degree of fusion, chosen response and later outcome. Over time, this reveals recurring patterns and helps distinguish contemplative insight from vague impressions.
Trauma-sensitive practice may require shorter sessions, open eyes, freedom to move, external anchors, predictable instructions and explicit permission to stop. No practitioner should be pressured to remain with overwhelming sensations. Choice is not a concession to the practice; restoration of choice is one of its purposes.
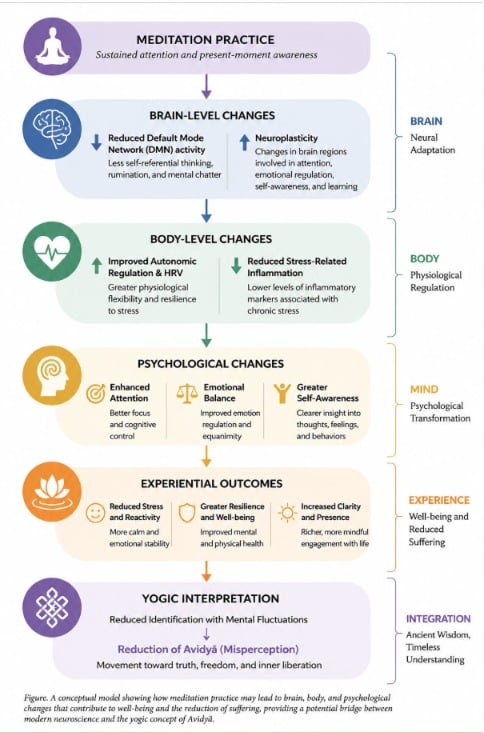
What Might Be Happening in the Brain and Body?
Neuroscience can investigate the correlates of meditation, but it should not be used as decorative proof of ancient metaphysics. Meditation is not a single intervention. Focused attention, open monitoring, mantra repetition, compassion practice, movement-based Yoga and nondual contemplation employ different instructions and may produce different states. Results from one form cannot automatically be generalised to every other form.
The Default Mode Network. The Default Mode Network, or DMN, includes hubs in the medial prefrontal cortex, posterior cingulate cortex and precuneus, with additional involvement of angular and temporal regions. It participates in autobiographical memory, self-referential processing, social cognition, future simulation and spontaneous thought. It is therefore misleading to call it merely the brain’s “ego network” or to assume that less activity is always healthier.
Some meditation studies report altered DMN activity or connectivity, particularly in relation to attention and self-referential processing. A meta-analysis of resting-state connectivity found modest changes between nodes of the DMN, salience network and frontoparietal control network following mindfulness training. The emerging account is not simply that meditation switches the DMN off. It may alter how self-generated thought is monitored and how attention returns from mind-wandering.
Salience and control networks. The anterior insula and dorsal anterior cingulate contribute to detecting behaviourally relevant events, while frontoparietal systems support attention and cognitive control. Training may improve recognition that the mind has wandered and facilitate a less reactive return to the chosen object. This network interaction offers one possible biological correlate of meta-awareness, but the mapping remains probabilistic rather than one-to-one.
Autonomic regulation and heart rate variability. Heart rate variability, or HRV, describes variation in the intervals between heartbeats. Certain measures reflect aspects of parasympathetic regulation, but HRV is affected by breathing rate, posture, fitness, age, medication and measurement procedures. Contrary to confident popular claims, a meta-analysis of 19 randomised trials found insufficient evidence that predominantly seated mindfulness interventions reliably increased resting vagally mediated HRV compared with controls. Slow breathing can alter HRV acutely, so breathing effects must also be separated from meditation-specific effects.
Stress physiology and inflammation. Chronic stress can affect the hypothalamic-pituitary-adrenal axis, sleep, immune signalling and health behaviour. Some studies associate contemplative interventions with changes in cortisol or inflammatory markers such as C-reactive protein and pro-inflammatory cytokines. However, a systematic review combining HRV and inflammatory outcomes found mixed and inconclusive results. It is therefore reasonable to investigate these pathways, but premature to promise that meditation will “switch off inflammation.”
Neuroplasticity. Learning of any kind can modify brain function, and sustained practice may be associated with structural or functional changes in regions involved in attention, interoception and regulation. A grey-matter meta-analysis found the most consistent structural result in the right anterior ventral insula, while also identifying weak statistical power and risks of selection, attrition and confirmation bias across the literature. Structural differences in experienced meditators may reflect training, pre-existing traits, lifestyle or all three.
These limitations do not make contemplative neuroscience uninformative. They establish the standards required for credible interpretation: adequate sample sizes, active control groups, preregistration, correction for multiple comparisons, replication, measurement of adverse effects and precise description of the practice. A colourful scan cannot by itself demonstrate healing, enlightenment or a consciousness independent of the brain.
A Transdiagnostic Account of Suffering
Diagnostic categories remain important because different disorders involve different risks, courses and treatments. At the same time, several processes cut across diagnoses: rumination, worry, attentional capture, cognitive fusion, experiential avoidance, sleep disruption, shame, behavioural withdrawal and difficulty regulating arousal. These processes may help explain why related skills can support people with otherwise different problems.
Sākṣī Bhāva can be interpreted as a way of changing the relationship to these processes. Rumination becomes observable repetition rather than mandatory problem-solving. An intrusive thought becomes an unwanted event rather than evidence of character. Pain remains physically real but may become less entangled with catastrophic prediction. An emotion becomes information and energy requiring wise response, not an identity that must dictate behaviour.
This transdiagnostic potential must not be exaggerated. Mania, psychosis, severe major depression, obsessive-compulsive disorder, eating disorders, substance dependence, neurodevelopmental conditions and trauma-related disorders may require highly specific assessment and intervention. Witnessing practice may serve as one component of care, may need substantial adaptation or may be temporarily inappropriate.
An Integrated Model for Mental Health Care
A responsible synthesis can be organised into five interacting layers. The first is clinical assessment and safety: diagnosis where appropriate, evaluation of suicide risk, screening for medical contributors, review of medication, and attention to substance use, sleep and trauma. Without this foundation, contemplative language can obscure urgent needs.
The second layer is evidence-based treatment. Depending on the condition, this may include psychotherapy, medication, family intervention, rehabilitation, occupational support or hospital care. Meditation should not be used to pressure someone into avoiding indicated treatment, and prescribed medication should not be stopped or altered without guidance from the relevant clinician.
The third layer is contemplative skill. Practices of attention, witnessing, ethical reflection, compassion and equanimity may strengthen the capacity to participate in treatment and respond to distress. Their role is generally complementary, not competitive.
The fourth layer is embodied regulation. Sleep, nutrition, movement, breathing, exposure to daylight, treatment of physical illness and reduction of harmful substance use directly affect mental functioning. This is where Yoga and carefully evaluated Ayurvedic lifestyle insights may enter dialogue with behavioural medicine, provided that safety, evidence quality and individual context remain explicit.
The fifth layer is relational and structural. Family support, meaningful work, financial security, safe housing, freedom from violence, community belonging and access to care shape mental health. No account of witness-consciousness should convert social injustice into an individual failure to remain calm. Inner freedom and collective responsibility must be treated as complementary obligations.
Safety, Contraindications and Ethical Teaching
Meditation and mindfulness are often low-risk, but they are not risk-free. The United States National Center for Complementary and Integrative Health notes that adverse experiences have been insufficiently studied; a review cited by the agency estimated negative effects in approximately 8% of participants, most commonly anxiety and depression. Risk may depend on the technique, intensity, setting, teacher competence and participant history.
Extra caution is appropriate for people experiencing acute psychosis, mania, severe dissociation, destabilising trauma symptoms, intense panic, profound sleep loss or active suicidal thinking. Long retreats, sensory deprivation, aggressive breath manipulation and repeated assertions that the body or world is unreal can be especially destabilising for some individuals. Clinical collaboration and gradual, grounded practice are preferable to heroic intensity.
Ethical instruction should include informed consent, permission to stop, transparent limits of teacher competence, referral pathways and explicit reporting of adverse events. A teacher should not diagnose psychiatric conditions without qualifications, discourage medical care or interpret deterioration as proof that a practice is “working.”
If a person is at immediate risk of self-harm, unable to remain safe or losing contact with reality, contemplative self-help is not an adequate response. Urgent assistance from local emergency services, a crisis service or a qualified mental health professional is required.
A Research Agenda for Sākṣī Bhāva
The scientific study of Sākṣī Bhāva begins with construct clarity. Researchers must specify whether they are measuring meta-awareness, disidentification, nonreactivity, attentional stability, equanimity, self-as-context or a tradition-specific realisation. Combining these into an undefined “witness score” would produce apparent precision without conceptual validity.
Interventions should then be described in replicable detail: instructions, duration, teacher training, philosophical framing, home practice, breathing components, movement, group support and safeguards. A study of ten minutes of guided observation cannot be casually generalised to intensive contemplative discipline, and results from experienced practitioners cannot be assumed to apply to beginners.
Trials require appropriate comparison conditions. Wait-list controls can exaggerate apparent benefit because they do not control for expectation, instructor attention or group belonging. Active controls, adequate statistical power, preregistration, intention-to-treat analysis and long-term follow-up would permit stronger causal inference. Benefits and harms should be reported with equal seriousness.
Measurement should operate across levels. Self-report can assess fusion, rumination and well-being; behavioural tasks can examine attentional flexibility; ecological sampling can capture daily functioning; physiological measures can assess arousal; and neuroimaging can test specific network hypotheses. Clinical outcomes should include functioning, relapse, quality of life and treatment engagement, not only short-term reductions in questionnaire scores.
Cultural fidelity is equally important. Sanskrit and Tamil concepts should not be stripped of context merely to make them resemble familiar Western constructs. Scholars of Yoga, Vedānta, Ayurveda, Siddha and other relevant traditions should participate in study design alongside clinicians, neuroscientists, statisticians and people with lived experience. Dialogue is methodologically stronger than extraction.
Research in India must also address linguistic diversity, rural and urban differences, caste and economic inequalities, local explanatory models, treatment gaps and the availability of trained personnel. Digital delivery may expand access, but an application cannot reliably assess every contraindication or replace human care in complex cases. Scale should not be purchased at the cost of safety.
The Road Ahead
The future of mental health care does not require a contest in which ancient wisdom defeats modern science or science dismisses contemplative knowledge. Indian Knowledge Systems preserve sophisticated inquiries into attention, embodiment, suffering, conduct and consciousness. Contemporary medicine contributes diagnostic precision, controlled evaluation, crisis care and methods for identifying both benefit and harm. Each can expose the blind spots of the other.
The central insight of Sākṣī Bhāva is modest in expression but potentially far-reaching in practice: a person is not reducible to the most painful thought, strongest emotion, most frightening memory or current social role. Experiences arise within awareness, influence behaviour and deserve appropriate response, yet they need not become total definitions of identity.
For someone caught in anxiety, this distinction may create enough space to test a catastrophic prediction. For someone vulnerable to depressive rumination, it may reveal that the mind is repeating an old pattern rather than delivering a final verdict. For someone grieving, it may permit sorrow to remain profound without making the future logically impossible. These are not miraculous cures. They are increments of freedom, and increments of freedom can alter the direction of a life.
The most defensible conclusion is therefore neither romantic nor dismissive. Witness-consciousness deserves careful clinical adaptation and rigorous research as a possible transdiagnostic skill, embedded within ethical, embodied and evidence-based care. Its deepest contribution may be the recovery of perspective: distress is real, treatment matters, circumstances matter, and awareness can learn to meet experience without becoming completely imprisoned by it.
This discussion is educational and does not provide diagnosis or individual medical advice.
Selected Evidence
Global prevalence and burden: GBD 2023 Mental Disorder Collaborators, The Lancet (2026); and the World Health Organization mental disorders fact sheet.
India-specific estimates: India State-Level Disease Burden Initiative Mental Disorders Collaborators, The Lancet Psychiatry (2020).
Meditation effectiveness and safety: National Center for Complementary and Integrative Health.
Decentering and related processes: Bernstein and colleagues, critical review and metacognitive processes model.
Default Mode Network connectivity: Rahrig and colleagues, systematic review and meta-analysis.
HRV, inflammatory markers and structural neuroimaging: Brown and colleagues on HRV, Rådmark and colleagues on physiological markers, and Pernet and colleagues on grey-matter findings.
Inspired by this post on Indica Today.










Leave a Reply
You must be logged in to post a comment.